
A correspondent writes:
I assumed you would possibly care to touch upon a rebuttal in at the moment’s HealthAffairs. I discover it a poor non-defense that depends on “1000s of research used our measure and located it legitimate”, in addition to assaults on the critics of their work.
The difficulty started when the Middle of Medicare & Medicaid Companies (CMS) determined to discover a well being fairness cost mannequin referred to as ACO-REACH. CMS selected a income impartial scheme to take away some {dollars} from funds to suppliers serving the most-advantaged individuals and re-allocate these {dollars} to probably the most deprived. In fact, CMS wants to decide on a measure of poverty that’s 100% obtainable and simple to compute. These necessities restrict the measure to a poverty index obtainable from Census knowledge.
CMS selected to make use of a typical poverty index, College of Wisconsin’s Area Deprivation Index (ADI). Issues received spicy earlier this yr when another researchers noticed that no areas within the Bronx or south-eastern DC are within the lowest deciles of the ADI measure. After digging into the ADI strategies a bit deeper, it appears the difficulty is that the ADI doesn’t scale the housing {dollars} appropriately earlier than utilizing that part in a principal parts evaluation to create the poverty index.
One factor I discover perplexing in regards to the rebuttal from UWisc is that it fully ignores the existence of each different validated poverty measure, and particularly the CDC’s Social Vulnerability Index. Their rebuttal pretends that there isn’t a various resolution obtainable, and subsequently the ADI measure have to be used as is. Lastly, whereas ADI is publicly obtainable, it’s obtainable beneath a non-commercial license so it’s a bit deceptive for the authors to not disclose that they too have a monetary curiosity in pushing the ADI measure whereas accusing their critics of economic incentives for his or her criticism.
The opinions expressed listed here are my very own and don’t replicate these of my employer or anybody else. I would favor to stay nameless should you determine to report this to your weblog, as I want to not tie these private views to my employer.
Attention-grabbing. I’d by no means heard of any of this.
Right here’s the background:
Dwelling in a deprived neighborhood has been linked to various healthcare outcomes, together with increased charges of diabetes and heart problems, elevated utilization of well being companies, and earlier death1-5. Well being interventions and insurance policies that don’t account for neighborhood drawback could also be ineffective. . . .
The Space Deprivation Index (ADI) . . . permits for rankings of neighborhoods by socioeconomic drawback in a area of curiosity (e.g., on the state or nationwide stage). It consists of components for the theoretical domains of earnings, training, employment, and housing high quality. It may be used to tell well being supply and coverage, particularly for probably the most deprived neighborhood teams. “Neighborhood” is outlined as a Census block group. . . .
The rebuttal
Clicking on the above hyperlinks, I agree with my correspondent that there’s one thing bizarre in regards to the rebuttal article, beginning with its title, “The Space Deprivation Index Is The Most Scientifically Validated Social Exposome Instrument Accessible For Insurance policies Advancing Well being Fairness,” which elicits recollections of Chilly-Conflict-era Pravda, or maybe an Onion article parodying the thought of somebody protesting an excessive amount of.
The article continues with some enjoyable buzzwords:
This yr, the Middle for Medicare and Medicaid Innovation (CMMI) took a ground-breaking step, creating coverage aligning with multi-level fairness science and focusing on sources primarily based on each individual-level and exposome (neighborhood-level) drawback in a cost-neutral manner.
This kind of bureaucratic language shouldn’t in itself be taken to suggest that there’s something incorrect with the Space Deprivation Index. A profitable software on this area will get utilized by all kinds of businesses, and paperwork will unavoidably spring up round it.
Let’s learn additional and see how they reply to the criticism. Right here they go:
Hospitals situated in excessive ADI neighborhoods are typically hit hardest financially, suggesting well being fairness aligned insurance policies could supply them a lifeline. But lately, CMS has been criticized for choosing ADI to be used in its HEBA. In keeping with behavioral economics concept, potential losers will at all times struggle tougher than potential winners, and in a budget-neutral innovation like ACO REACH there are a few of each.
I’m unsure the behavioral economics framing is sensible right here. Completely different measures of deprivation will correspond to totally different hospitals getting additional funds, so in that sense either side within the debate symbolize potential winners and losers from totally different insurance policies.
They proceed:
CMS have to be allowed time to guage this system to find out what refinements to its methodology, if any, are wanted. CMS has signaled openness to fine-tune the HEBA if wanted sooner or later. In the end, CMS is right to behave now with the instruments of at the moment to advance well being fairness.
Positive, however then you can use one of many different obtainable indexes, such because the Social Deprivation Index or the Social Vulnerability Index, proper? It appears there are two questions right here: first, whether or not to institute this new coverage to “incentivize medical teams to work with low-income populations”; second, whether or not there are any obtainable measures of deprivation that make sense for this objective; third, if multiple measure is offered, which one to make use of.
So now on to their protection of the Space Deprivation Index:
The NIH-funded, publicly availably ADI is an extensively validated neighborhood-level (exposome) measure that’s tightly linked to well being outcomes in almost 1000 peer-reviewed, impartial scientific publications; is probably the most generally used social exposome measure inside NIH-funded analysis at the moment; and undergoes a rigorous, multidisciplinary analysis course of annually previous to its annual replace launch. Residing in excessive ADI neighborhoods is tied to organic processes akin to accelerated epigenetic getting older, elevated illness prevalence and elevated mortality, poor healthcare high quality and outcomes, and plenty of different well being components in analysis research that span the total US.
OK, so ADI is nationally correlated with varied dangerous outcomes. This doesn’t but handle the priority of the measure having issues domestically.
However they do get into the main points:
A latest peer-reviewed article argued that the financial values within the ADI needs to be re-weighted and an accompanying editorial famous that, as a result of these have been “variables that have been measured in {dollars},” they made parts of New York State seem much less deprived than the authors argued they need to be. But New York State normally is a really well-resourced state with one of many ten highest per capita incomes within the nation, mirrored of their Medicaid Federal Medical Help Proportion (FMAP). . . .
Some critics counting on face validity declare the ADI doesn’t carry out “effectively” in cities with excessive housing prices like New York, and likewise California and Washington, DC, and recommend {that a} re-weighted new model be created, once more ignoring proof demonstrating the sturdy hyperlink between the ADI and well being in all types of cities together with New York (additionally right here), San Francisco, Houston, San Antonio, Chicago, Detroit, Atlanta, and plenty of others. . . .
That first paragraph doesn’t actually handle the query, because the issues in regards to the South Bronx not having a excessive deprivation index are about one a part of New York, not “New York State normally.” However the rebuttal article does supply two hyperlinks about New York particularly, so let me have a look:
Given the bimodal distribution of ADI percentiles within the present pattern, the variable was analyzed in three teams: low (90–100), center (11–89), and excessive neighborhood SES.
To get a way of issues, I went to the web Neighborhood Atlas and grabbed the map of nationwide percentiles for New York State:
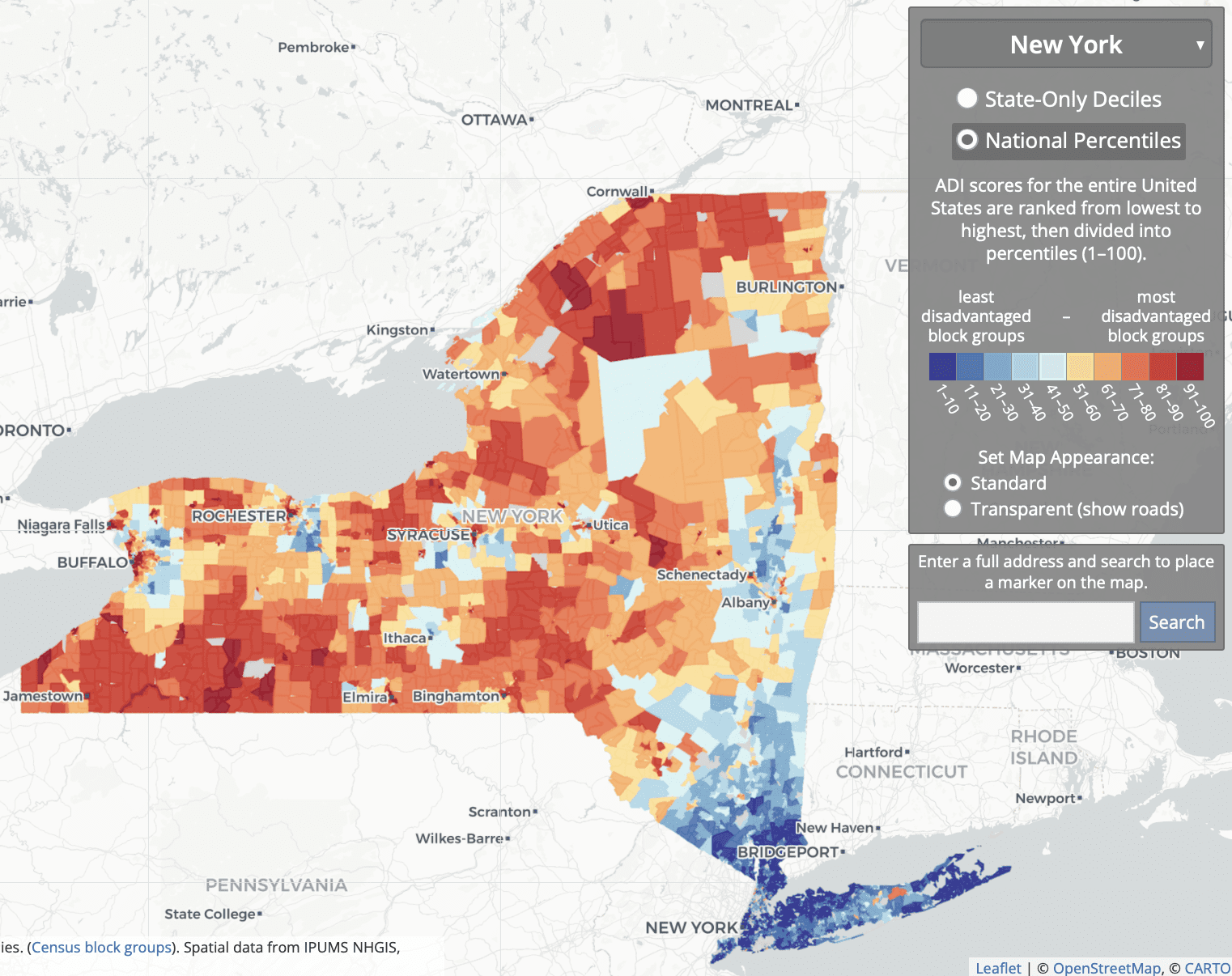
So what they’re doing is evaluating some wealthy areas of NYC and its suburbs; to some low- and middle-income components of town, suburbs, and upstate; to some low-income rural and inner-city areas upstate.
Association Between Residential Neighborhood Social Conditions and Health Care Utilization and Costs:
Retrospective cohort research. Medicare claims knowledge from 2013 to 2014 linked with neighborhood social circumstances on the US census block group stage of 2013 for 93,429 Medicare fee-for-service and dually eligible sufferers. . . . Deprived neighborhood circumstances are related to decrease whole annual Medicare prices however increased doubtlessly preventable prices after controlling for demographic, medical, and different affected person traits. . . . We restricted our pattern to sufferers with 9-digit residential zip codes obtainable in New York or New Jersey . . .
I don’t see the relevance of those correlations to the criticisms of the ADI.
To return to our fundamental thread, the rebuttal summarizes:
The ADI is presently probably the most validated scientific software for US neighborhood stage drawback. This doesn’t imply that different measures could not finally additionally meet this excessive bar.
My downside right here is with the time period “most validated.” I’m unsure how one can take this, given that each one this validation didn’t appear to have proven that downside with the South Bronx and many others. However, positive, I get their normal level: When doing analysis, higher to go together with the satan , and many others.
The rebuttal authors add:
CMS ought to proceed to analyze all choices, watch out for conflicts of curiosity, and keep the observe of vetting scientific validated, evidence-based standards when deciding on a software for use in a federal program.
I feel we are able to all agree on that.
Past normal defenses of the ADI on the grounds that many individuals use it, the rebuttal authors make an attention-grabbing level about using neighborhood-level measures extra typically:
Neighborhood-level socioeconomic drawback is simply as (and is typically extra) necessary than particular person SES. . . . These components don’t at all times overlap, one could also be excessive, the opposite low or vice versa. Each are critically necessary in equity-focused intervention and coverage design. Of their HEBA, as aligned with scientific observe, CMS has included certainly one of every—the ADI captures neighborhood-level components, and twin Medicare and Medicaid eligibility represents an individual-level issue. But teams have mistakenly conflated individual-level and neighborhood-level components, wrongly suggesting that neighborhood-level components are solely used as a result of further particular person components aren’t available.
They hyperlink to a review article. I didn’t see the reference there to teams claiming that neighborhood-level components are solely used as a result of further particular person components aren’t available, however I solely checked out that linked article rapidly so I in all probability missed the related quotation.
The above are all normal factors in regards to the significance of utilizing some neighborhood-level measure of drawback.
However what in regards to the particular issues raised with the ADI, such because the labeling many of the South Bronx as being low drawback (within the tenth to thirtieth percentile nationally)? Right here’s what I may discover within the rebuttal:
These assertions depend on what’s been described as “the weakest of all potential arguments”: face validity—outlined as the looks of whether or not or not one thing is an accurate measurement. That is in distinction to empirically-driven checks for assemble validity. Validation consultants universally discredit face validity arguments, classifying them as not professional, and extra aligned with “advertising to a constituency or the politics of evaluation than with rigorous scientific validity proof.” Face validity arguments on their very own are merely not adequate in any rigorous scientific argument and are fraught with potential for bias and battle of curiosity. . . .
Re-weighting suggestions run the danger of undermining the power and scientific rigor of the ADI, as any altered ADI model now not aligns with the highly-validated unique Neighborhood Atlas ADI methodology . . .
Some have urged that neighborhood-level drawback metrics be adjusted to particular wants and areas. We take into account this kind of change—re-ranking ADI into smaller, customized geographies or including native changes to the ADI itself—to be a kind of gerrymandering. . . . A call to customise the HEBA method in sure geographies or components of sure forms of places will profit some areas and disservice others . . .
I disagree with the declare that face validity is “the weakest of all potential arguments.” For instance, saying {that a} methodology is nice as a result of it’s been cited hundreds of occasions, or saying that native estimates are nice as a result of the nationwide or state-level correlations look proper, these are weaker arguments! And if validation consultants universally discredit face validity arguments . . . ummmm, I’m unsure who’re the validation consultants on the market, and in any case I’d wish to see the proof of this purportedly common view. Do validation consultants universally suppose that North Korea has reasonable electoral integrity?
The criticism
Right here’s what the important article lists as limitations of the ADI:
Utilizing nationwide ADI benchmarks could masks disparities and should not successfully seize the necessity that exists in among the increased cost-of-living geographic areas throughout the nation. The ADI is a relative measure for which included variables are: median household earnings; p.c beneath the federal poverty stage (not adjusted geographically); median residence worth; median gross hire; and median month-to-month mortgage. In some geographies, the ADI serves as an affordable proxy for figuring out communities with poorer well being outcomes. For instance, many rural communities and lower-cost city areas with low life expectancy are additionally recognized as deprived on the nationwide ADI scale. Nonetheless, for components of the nation which have excessive property values and excessive price of residing, utilizing nationwide ADI benchmarks could masks the inequities and poor well being outcomes that exist in these communities. . . .
They suggest “adjusting the ADI for variations in price of residing,” “recalibrating the ADI to a extra native stage,” or “making use of an absolute measure akin to life expectancy fairly than a relative measure such because the ADI.”
There appear to be two various things occurring right here. The primary is that ADI is a socioeconomic measure, and it may additionally make sense to incorporate a measure of well being outcomes. The second is that, as a socioeconomic measure, ADI appears to have issue in areas which can be low earnings however with excessive housing prices.
My abstract
1. I agree with my correspondent’s electronic mail that led off this publish. The criticisms of the ADI appear legit—certainly, they remind me a little bit of the Human Growth Index, which a similar problem of giving unreasonable summaries that may be attributed to somebody developing a reasonable-seeming index after which not trying into the main points; see here for extra. There was additionally the horrible, horrible Electoral Integrity Index, which had related problems with face validity that might be traced again to elementary problems with measurements.
2. I additionally agree with my correspondent that the rebuttal article is dangerous for a number of causes. The rebuttal:
– doesn’t ever handle the substantive objections;
– doesn’t appear to acknowledge that, simply because a measure provides cheap nationwide correlations, that doesn’t imply that it will probably’t have severe native issues;
– leans on an argument-from-the-literature that I don’t purchase, partially out of normal mistrust of the literature and partially as a result of not one of the cited literature seems to deal with the issues on the desk;
– presents a ridiculous argument towards the idea of face validity.
Face validity—what does that imply?
Let me elaborate upon that final level. When a technique produces a outcome that appears “on its face” to be incorrect, that doesn’t essentially inform us that the tactic is flawed. If one thing contradicts face validity, that tells us that it contradicts our expectations. It’s a shock. One risk is that our expectations have been incorrect! One other risk is that there’s a downside with the measure, through which case the contradiction with our expectations can assist us perceive what went incorrect. That’s how issues went with the political science survey that claimed that North Korea was a reasonably democratic nation, and that’s how issues appear to be going with the Space Deprivation Index. Even when it has hundreds of citations, it will probably nonetheless have flaws. And on this case, the critics appear to have gone in and located the place among the flaws are.
On this specific instance, the authors of the rebuttal have a number of choices.
They might settle for the criticisms of their methodology and attempt to do higher.
Or they might make the affirmative case that each one these components of the South Bronx, southeast D.C., and many others., aren’t truly socioeconomically disadvantaged. As a substitute they form of query that these areas are disadvantaged (“New York State normally is a really well-resourced state”) however with out fairly making that declare. I feel one cause they’re caught within the center is politics. Public well being is generally coming from the left facet of the political spectrum and, from the left, if an space is poor and has low life expectancy, you’d name it disadvantaged. From the proper, you can argue that these poor areas already get tons of presidency assist and that each one this welfare dependence simply compounds the issue. From a conservative perspective, you would possibly argue that these kinds of poor neighborhoods aren’t “disadvantaged” however fairly are already oversaturated with authorities assist. However I don’t suppose we’d be seeing a lot of that argument within the health-disparities area.
Or they might make a content-low response with out addressing the issue. Sadly, that’s the choice they selected.
I’ve no cause to suppose they’ve chosen to reply poorly right here. My guess is that they’re soooo comfy with their measure, soooooo positive it’s proper, that they only dismissed the criticism with out ever desirous about it. Which is simply too dangerous. However now they’ve this publish! Not too late for them to do higher. Tomorrow’s one other day, hey!
P.S. My correspondent provides:
The unique article criticizing the ADI measure has some map graphic sins that any editor ought to have eliminated earlier than publication. Listed here are some cleaner comparisons of town knowledge. The SDI measure in these plots is the Social Deprivation Index from Robert Graham Middle.
Washington, D.C.:
New York Metropolis:
Boston:
San Francisco space:




















{kind=link}